The Roles Played by Pharmaceuticals

Within the first few hours of seeing my father, I observed that he felt better in the mornings and would eat a little breakfast. Then after they gave him his crushed-up medications, he would feel miserable and not eat the rest of the day. I knew not eating wasn’t going to help him regain his strength.
After the third request, I finally received my father’s list of medications. There were 34 items on his list! Some of the items were over-the-counter drugs, vitamins, and minerals, but 20 of them were prescription drugs. I spoke to my father’s doctor about reducing them. Fortunately, he was receptive. Within 24 hours my father’s color was better and he started eating more.
Polypharmacy in the Elderly
Sadly, my father’s case of “polypharmacy” is not uncommon. Typically, as people age, their levels of key nutrients, hormones, enzymes, and antioxidants decrease while the number of prescription drugs taken increases. These changes can also be observed in the chronically ill.

Polypharmacy in those older than 65 years (“older adults”) is defined as taking multiple prescription medications at the same time. A 2010 review by Rochron and Gurwitz found 81-year-olds take an average of 15 different medications at one time. The range was from 6 to 28 medications.1
Data from the Center for Disease Control (CDC) for 2013-2016 indicate 64.8% of those 65 and older had taken three or more prescription drugs in the last 30 days and 40.9% had taken five or more. The percentage that had taken five or more increased almost three-fold from 1988-1994.2
Each additional medication makes an older adult more susceptible to drug reactions and interactions. Reactions can be subtle, such as restricted activity or overt, like a fall with hip fracture. Polypharmacy is a risk factor for physical and cognitive decline and reduced independence.3
Sometimes, like in my father’s case, polypharmacy creeps in when multiple doctors are prescribing. My father’s cardiologist decided a statin wasn’t appropriate for Dad after he experienced side effects. His VA doctor then prescribed one, and Dad took it without even knowing what he was taking.
The Prescription Cascade Merry-Go-Round

Because prescription drugs pass through your digestive system, side effects may include stomach problems like nausea, diarrhea, and constipation. Other side effects may include dizziness, drowsiness, depression, irritability, weight gain, or a disruption in your sleep or sex drive. There are far too many possible side effects to list here.
I review all drugs my clients take for drug-nutrient interactions. I don’t want to recommend any foods or supplements that would interact with their medications. I also look at drug-to-drug interactions and side effects. That tells me if we’ll be swimming upstream with the work we’re trying to do. I’ve never not seen manifested side effects and/or listed drug interactions if a client is taking more than four or five drugs. Some drugs like gabapentin interact with many other drugs, but I see them prescribed together anyway. Therefore, I don’t work with clients taking more than three drugs unless they’re working with a physician to reduce the need for that many prescriptions. When you address the root cause of a condition and support the body to function as designed, that many drugs are seldom needed.
Ponte et al. in their 2017 paper wrote: “Since futile polymedication enhance the chances of developing new diseases, the resulting polypharmacy represents a major health risk, raises senseless health costs, and generates potentially preventable morbidity and mortality.4
Chronological Age Does Not Determine Vulnerability
Age-blaming is not empowering and assumes there’s nothing you can do about being vulnerable. We need to look beyond chronological age and examine factors that differ between the young and the old – factors

As I write this, we are in the midst of a pandemic caused by SARS-CoV-2, commonly known as “the Coronavirus”. The pandemic has spread to every continent except Antarctica. Widespread fear has spread along with the virus because the virus is hyped as being highly “contagious”.
I credit my friend and mentor Dr. Alex Vasquez for teaching me this truth: A virus isn’t contagious without a hospitable/vulnerable host. Just as cancer needs a hospitable environment/body in which to grow, a virus needs a hospitable host to help it replicate. We all have cancer cells and numerous viruses in our body at any given time, but if your immune system is functioning properly, it keeps them from harming you. As you may know, people can spread a virus without being sick or even knowing they have it. That’s because the host determines a virus’s effect. In other words, your immune system is more important than the contagiousness of a virus.
Data shows the vast majority of those who die from COVID-19 (the disease caused by SARS-CoV-2) are older people and those with underlying health conditions (comorbidities). Those conditions include lung disease (often caused by smoking), high blood pressure, cardiovascular disease, severe obesity, diabetes, kidney failure, and liver disease. Azra Ghani, from Imperial College London said in a journal news release, “Our analysis very clearly shows that at age 50 and over, hospitalization is much more likely than in those under 50, and a greater proportion of cases are likely to be fatal.”
Ghani’s statement, taken alone, could be very disempowering. I’m over 50, but as my friend and mentor Jeff Herring says, “Elderly is always about 15 years older than me.” Age is relative but undeniable. I was shocked when I heard Italian hospitals weren’t giving ventilators to anyone with COVID-19 over 60 years old because I’m also over 60! I’m healthy and don’t have any “underlying” conditions, but I can’t say the same for some of my friends and family members.
If age is to blame for COVID-19 mortality, how do we count for survivors like
- Zhang Guangfen, from Wuhan, China, age 103
- P, from Italy, age 103
- Ada Zanusso, from Italy who also survived the Spanish Flu, age 104
- Bill Lapschies, from Oregon who also survived the Spanish Flu, age 104
- Connie Titchen, from Great Britain, age 106
- Cornelia Ras, from the Netherlands, age 107
- Rudolph Heider, from Missouri who also survived the Spanish Flu, age 107
- Sylvia Goldsholl, a New Jersey nursing home resident, age 108
- Maria Branyas, a care-home resident from Spain, age 113
These people may be outliers. They are also shining examples of why we can’t just look at age as a number and blame chronological age for vulnerability.
Drug-Induced Nutrient Depletion
While pharmacists are expected to check interactions between prescriptions, they don’t commonly consider drug-induced nutrient depletion.5 Prescription drugs can deplete nutrients in various ways by

- interfering with absorption
- decreasing appetite
- blocking enzymes necessary for production
- blocking a nutrient’s effects at the level of the cell
- increasing loss of nutrients through your urinary system.
For simplicity, I use the term “drug mugging” from pharmacist Suzy Cohen’s book Drug Muggers to describe any process by which drugs deplete nutrients. The book is an excellent resource if you want to investigate the topic further.
Polypharmacy, the prescribing cascade, and drug mugging are just a few modifiable factors that can weaken the immune system and increase vulnerability. It doesn’t have to be like this. We can and need to do better. A functional medicine approach that identifies and addresses the root cause of disease rather than continuously masking symptoms with prescriptions would significantly reduce this problem.
Depleted Nutrients, Hormones, Antioxidants, and Enzymes
Drugs, as well as aging, a poor diet and/or malabsorption of nutrients can result in deficiencies or insufficiencies in the body that cause the immune system to function poorly. These deficiencies often go unrecognized and thus, unaddressed.
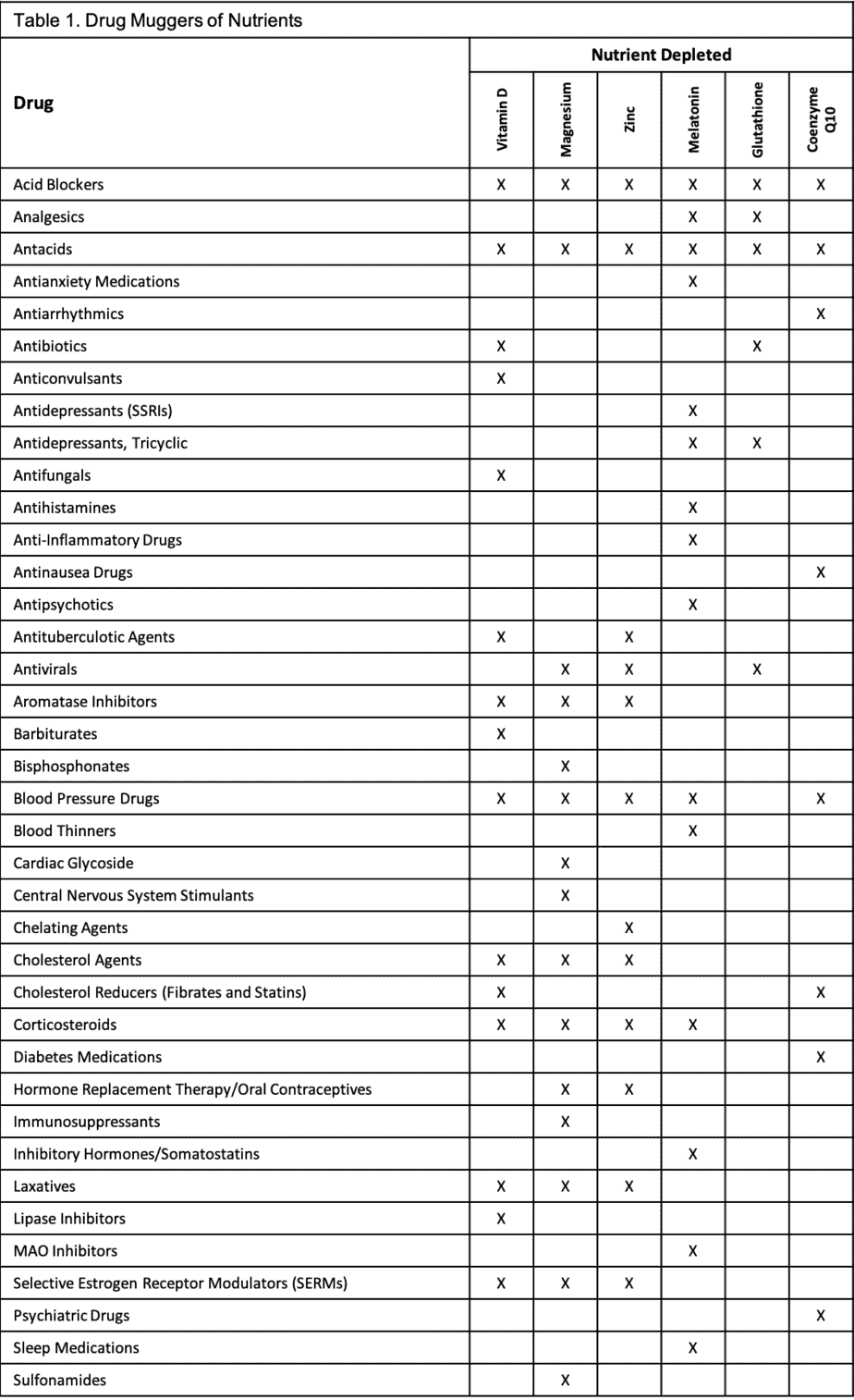
In the following material, I use the term “drug mugging” from pharmacist Suzy Cohen’s book Drug Muggers to describe drug-induced nutrient depletion. I listed categories of drugs as “drug muggers” rather than brand names. These drug muggers are summarized in Table 1. Not all drugs in a specific category have the same effects, so you should talk to your doctor and/or pharmacist about your specific medications. If you’re taking a drug and don’t know the class it fits into or what it does, you need to know. Knowledge is power so do your homework and step into that power.
The nutrients included in Table 1 are just those discussed here. The listed drugs may deplete other nutrients. For example, in addition to depleting vitamin D and coenzyme Q10, statins deplete vitamins A, B12, E, K, beta-carotene, folic acid, and iron.6
Vitamin D – Vitamin D has an important role in bone health and is critical for immune function and reducing inflammation. Without enough vitamin D, the body can’t make antimicrobial peptides (part of the innate immune system that can kill bacteria, viruses, fungi, and cancer cells).7
Evidence exists that Vitamin D deficiency can decrease lung function8 and vitamin D3 supplementation can reduce mortality in older adults.9
Vitamin D deficiency can masquerade as fibromyalgia, depression, and chronic fatigue syndrome.10 At least 80% of the elderly are vitamin D deficient, putting them in a perpetual state of immune suppression.
I struggle with low

Vitamin D is sometimes called the “sunshine vitamin” because historically, vitamin D was obtained almost exclusively from the sun. The sun’s ultraviolet B (UVB) rays convert cholesterol in the skin to vitamin D3. The elderly may not get adequate sunlight exposure to make vitamin D if they’re shut in, have dark skin, or wear sunscreen. Reduced kidney function or magnesium deficiency may suppress activation of vitamin D, worsening a deficiency. The amount of “safe” and effective sun exposure depends on how far you are from the equator, the time of year, and the color of your skin. You don’t want to burn, so if you’re in the sun for a longer period, consider less toxic sunscreens such as those evaluated by the Environmental Working Group or you can make your own sunscreen with zinc oxide.
Vitamin D is a fat-soluble vitamin and is best absorbed in the intestine when bile and fat are present. Older adults may not be consuming enough healthy fats for optimal absorption. Decreased absorption may also be age-related, or due to
- iron deficiency
- chronic liver disease
- pancreatic insufficiency
- disease of the small intestine.
Drug muggers of vitamin D include acid blockers, antacids, antibiotics, anticonvulsants, antifungals, antituberculotic agents, aromatase inhibitors, barbiturates, bile salt sequestrants/cholesterol agents, calcium-channel blockers, cardiac glycoside, corticosteroids, diuretics, fibrates, hydroxychloroquine, laxatives, lipase inhibitors, Selective Estrogen Receptor Modulators (SERMS), and statins.
Magnesium – Magnesium is one of the most important micronutrients in the body. It has beneficial effects all over the body and participates in over 300 biochemical reactions. Magnesium plays a key role in the immune system – in both the innate and acquired immunity. Scientists believe magnesium deficiency contributes to the aging process and vulnerability to age-related diseases. Magnesium imbalance in older adults is also related to stress susceptibility and inflammation.11
The magnesium content of processed food is lower than in whole foods. Older adults are less likely than younger adults to consume enough magnesium from green leafy vegetables, whole grains, legumes, and nuts to meet their needs. With increasing age, physical activity declines along with food intake. Yet, magnesium requirements, remain the same.
Besides a poor diet, magnesium deficiency may also be caused by alterations in magnesium metabolism or drugs. Drug muggers of magnesium include acid blockers, antacids, aminoglycosides, amphotericin B, antibiotics, antipsychotics, antiviral agents, aromatase inhibitors, beta-2 antagonists, bisphosphonates, blood pressure drugs, cardiac glycoside, central nervous system stimulants, bile salt sequestrants/cholesterol agents, cisplatin, corticosteroids, cyclosporine, diuretics, immunosuppressants, hormone replacement therapy/oral contraceptives, levothyroxine, lithium, statins, SERMs, sulfonamides, and theophylline.
Zinc – Zinc is essential for both innate and acquired immunity. It is required to make protein and acts as an antioxidant. Antioxidants are like “anti-agers” because they help protect your cells from free radical or oxidative damage.
Low zinc status is commonly reported in the elderly. It impairs immune function and decreases resistance to pathogens. Even marginal zinc deficiency may cause inadequate responses to infections and immunosenescence (immune dysregulation associated with aging). Low zinc status is also a risk factor for pneumonia and mortality in the elderly.12,13
Zinc levels decline with age, with or without drug muggers. Absorption may be reduced in the elderly.13 Drug muggers of zinc include acid blockers, antacids, certain ACE inhibitors, angiotensin II receptor blockers, antituberculotic agents, antivirals, aromatase inhibitors, aspirin, blood pressure drugs, cholesterol agents, corticosteroids, diuretics, fibrates, hormone replacement therapy/oral contraceptives, laxatives, penicillamine, SERMs, and tetracyclines.
Melatonin – Melatonin is the sleep hormone. It is produced naturally from the amino acid tryptophan, by the pineal gland at night-time. Production of melatonin also requires vitamins B3 (niacin) and B6 (pyridoxine).
Melatonin doesn’t just help you sleep. It helps a variety of systems work properly, including the immune system. Melatonin acts on both innate and acquired immunity. Melatonin protects the structure and function of neurons and acts as an anti-inflammatory, antioxidant, anti-obese, and anti-aging agent.14
Melatonin levels increase steeply after the third month of life. Levels peak in early childhood and decline gradually by 10–15% per decade. By age 60, the pineal gland only produces negligible amounts of melatonin. This decline in melatonin, helps explain why older adults are more prone to infections as well as why their sleep patterns change. However, this decline does not appear to be a normal part of healthy aging. Researchers compared melatonin levels of 34 healthy, drug-free older men and women to a group of young men. They found no significant difference, concluding the decline is not part of healthy aging. It is likely due to poor health and/or medication use.15
Drug muggers of melatonin include acid blockers, antacids, analgesics, antianxiety medications, antidepressants, antihistamines, anti-inflammatory drugs, antipsychotics, blood pressure drugs (adrenergic receptor agonist- methoxamine, beta-blockers, calcium channel blockers, clonidine), corticosteroids, inhibitory hormones/somatostatins, MAO inhibitors, and sleep medications.
Glutathione – Glutathione is found in every cell in your body. It works to improve communication between the cells and to stabilize and protect them. It is sometimes called the “master antioxidant” because it is so good at protecting your cells from damage. Besides being a powerful antioxidant, glutathione is an anti-inflammatory agent and a powerful detoxifier.16
Glutathione is made in the liver using B vitamins, and three amino acids: glycine, glutamine, and cysteine. Older adults produce less glutathione due to insufficient amounts of amino acids, especially cysteine. Less glutathione means more oxidative stress in their cells.17
A study at Baylor School of Medicine found lower glutathione levels to be associated with less fat burning and more fat storing.18 Being overweight and obese is a common problem in the elderly. Excess abdominal fat increases the risk of obesity-associated immune disfunction and insulin resistance (meaning the cells don’t respond to insulin). Insulin resistance is linked to chronic inflammation and poor immune responses. When immune cells can’t sense and respond to insulin, they don’t do a good job of fighting pathogens.19
The Baylor researchers also found when they corrected age-associated glutathione deficiency, insulin sensitivity improved.18 Insulin resistance increases the risk of developing diabetes, heart disease, metabolic syndrome, and mortality. Thus, it is important to address glutathione deficiency and ensure your body has the amino acids available to make it.
Tylenol (acetaminophen) is one of the most commonly used drugs in the U.S. It is notorious for liver damage as well as depleting glutathione levels. It is not uncommon for older adults to take acetaminophen daily as an over-the-counter (OTC) or prescription drug. In 2011, to reduce the risk of liver damage and allergic reactions, the U.S. Food and Drug Administration (FDA) asked, but did not require, drug manufacturers to limit the dose of acetaminophen in products to 325 mg. At the same time, a Boxed Warning highlighting these risks became mandatory on the label of all prescription drugs containing acetaminophen.20
Glutathione levels in the body may be reduced by several factors, including poor nutrition, environmental toxins, and stress. Other drug muggers of glutathione include acid blockers, antacids, analgesics, antibiotics, antidepressants, and antivirals.
Coenzyme Q10 (CoQ10): CoQ10 is essential for life and for making energy in our bodies. CoQ10 increases resistance to infections, enhances immune function, and helps prevent immunosenescence (age-related decline in immune function).21-24 CoQ10 deficiency is associated with numerous diseases, including heart disease, cancer, and Alzheimer’s disease.
CoQ10 declines with age, accompanied by declines in energy metabolism. The body makes its own CoQ10, but the process is dependent on the same enzyme blocked by statin drugs. Because CoQ10 plays a role in muscle cell energy production, CoQ10 supplementation may help reduce statin-induced muscle pain.
Drug muggers of CoQ10 include acid blockers, antacids, antiarrhythmics, antibiotics, antidepressants (Tricyclic), antinausea drugs, blood pressure drugs, cholesterol reducers (fibrates and statins), diabetes medications, HIV drugs, and psychiatric drugs.
When a body is depleted and improperly nourished, it cannot heal. Anyone who thinks nutrition doesn’t make a difference doesn’t understand biochemistry.
Poor Nutrition in the Elderly
As people age, their eating habits change. They may no longer be able or willing to cook. My grandmother was an awesome cook and cooked for a large family for many years. I never saw my grandfather cook. I don’t remember exactly when it was, but Grandma reached a point when she said she was done cooking and she stopped. Sometimes older people aren’t mobile enough to cook or may be forgetful and thus unsafe while cooking.
Older adults often lose their appetite due to
- medications
- changes in smell or taste
- lack of physical activity
- depression
- illness
Poor dental health or difficulty swallowing or chewing can make eating difficult. Limited income or mobility can make access to healthy food difficult. Dietary restrictions and/or eating alone can make eating undesirable. Additionally, home-cooked meals and meals furnished by home delivery services such as Meals on Wheels may not be well-balanced.
For the above-listed reasons, many older adults are at risk of malnutrition, which can lead to
- a weak immune system, which increases the risk of infections
- muscle weakness, which increases the risk of falling
- decreased bone mass, which increases the risk of fractures
- an increased risk of death.
Boost and Ensure are commonly recommended as dietary supplements by the medical profession. These products are chemical concoctions with a form of sugar as their first ingredient, which lowers immunity. They are devoid of any “real” food ingredients. Boost and Ensure are marketed to healthcare professionals by Nestle and Abbott, but healthier alternatives are available. My favorite liquid meal replacement is PURE PALEOMEAL®. I love to mix half chocolate and half vanilla with coconut milk. I also bought dairy-free Orgain to nourish my husband prior to his surgery to fix his swallowing issue.
As mentioned previously, Meals on Wheels is another commonly recommended solution to curbing malnutrition. Meals on Wheels is great for feeding those who would otherwise not eat and for doing welfare checks on people. It might be a stretch to say their meals provide subsistence rather than sustenance; let’s just say they leave a lot to be desired. My mother became prediabetic after eating meals furnished by Meals on Wheels. She told me they ate a lot of pasta and dessert, so I reviewed one of their monthly meal plans. It was disturbing to see the amount of refined carbohydrates and sugars they were being fed. That month’s plan, which my mom said was typical, didn’t include any dark leafy greens – just iceberg lettuce six times during the month. Cruciferous vegetables were served only three times: broccoli, coleslaw, and then broccoli/cauliflower. Every meal included dessert – even when the meal also included fruit.
I couldn’t bear to look at any other month’s plans. I doubted I could change the program, so I started filling my parents’ freezer with healthy meals whenever I visited. My sister and I also gifted them Ice Age meals when they were on sale, as they frequently are. I encourage you to do whatever you can and make meals a social event whenever possible.
The Big Fat Lie
For years Americans were conditioned to believe that dietary fat was a bad thing and thus, many older adults are on a low-fat diet. While that may be the right diet if it was prescribed by a professional, it’s not for everyone. In fact, researchers in the Netherlands found people older than 85 with the highest cholesterol levels are best protected from cancer and infections.25
One of the problems with low-fat is that low-fat products often replace fat with empty calories from sugar or corn syrup to make up for the flavor and texture loss. Consuming empty calories from sugars increases the risk of diabetes and obesity. It’s more important to eat the right fats than to try and cut fat out of your diet. Fats/cholesterol are important for

- a healthy immune system
- brain health
- building healthy cell membranes
- making vitamin D and hormones
- controlling insulin.
Trans-fats (labeled as partially hydrogenated or hydrogenated oils) should always be avoided as should refined vegetable oils (like soybean, sunflower, canola, corn, safflower oil). The fats we need to get from our diet include:
- Saturated fats (long- and medium-chain) – Saturated fats help protect the liver from damage by toxins, chemicals, and prescription drugs. Medium-chain saturated fats such as lauric acid in coconut oil have antibacterial, antiviral, and antioxidant properties.
- Monounsaturated fats – Monounsaturated fats can help reduce bad cholesterol levels in your blood which can lower your risk of heart disease and stroke. They also provide nutrients to help develop and maintain your body’s cells. Good sources of monounsaturated fats include olives or olive oil, avocados, eggs, macadamia nuts, and almonds.
- Polyunsaturated fats – These are the heart-healthy omega-3 and omega-6 essential fatty acids that your body can’t make. Thus, you must consume them regularly from sources like wild-caught fatty fish and seafood like salmon, some grass-fed meats, high-quality eggs, nuts, seeds, green leafy veggies, and sea vegetables.
Other Vulnerability Factors in the Elderly
Chronic inflammation or infection – Inflammation is part of the body’s natural immune response to a stressor or injury. Initially, inflammation is beneficial, but when it becomes chronic it can perpetuate chronic disease and wear down the immune system. When it becomes excessive, it can be harmful and dangerous.
Nearly all degenerative diseases are diseases of inflammation. Cardiovascular disease, cancer, dementia, and diabetes all have inflammation as a common factor.
What’s at the end of your fork is the most likely contributor to chronic inflammation. Every bite of food is inflammatory or anti-inflammatory. Other common contributors to chronic inflammation include
- poor gut health
- dysbiosis (an imbalance in your microbiome)
- chronic stress
- autoimmune disease
- smoking
- obesity
- alcohol.
Stomach acid – Stomach acid is friend – not foe – unless you have acid reflux or GERD. Stomach acid is our first line of defense against ingested pathogens. If enough acid is present, the stomach’s acidic environment will kill invaders.
You need stomach acid for breaking down proteins and absorbing nutrients like calcium, magnesium, and zinc. If proteins are not broken down properly, they can trigger immune reactivity.
Acid r

While acid blockers or antacids may relieve the pain and prevent damage to tissue in the esophagus, they decrease the body’s ability to fight infection, digest foods and absorb nutrients. Because stomach acid decreases with age and acid-blocking medications are widely prescribed, the elderly are more prone to an increased risk of
- Clostridium difficile infection
- fractures
- community-acquired pneumonia
- vitamin B12 deficiency
- kidney disease
- dementia.27
If you or a loved one have acid reflux and are taking acid-reducing medication, I recommend addressing the root cause of acid reflux with a functionally-minded practitioner. Consider discussing the necessity of long-term use and/or possible alternatives.
Dehydration – Water is the most important nutrient in the body. It improves oxygen delivery to cells, moistens oxygen for easier breathing, lubricates joints, removes wastes, transports nutrients, flushes toxins, helps regulate body temperature, and prevents tissues from sticking.
Chronic dehydration is a common problem for many elderly people in the U.S. Older adults have a greater risk of dehydration because they have

- a lower volume of water in their bodies (Water comprises 75% of body weight in infants, but only 55% in the elderly.)
- a reduced ability to conserve water
- a diminished sense of thirst.28
Additionally, older adults may have conditions or take medications such as diuretics or laxatives that compound the problem. Thus, elderly people are more likely to become dehydrated during illnesses such as influenza, bronchitis, and those affecting the lungs or bladder.29
Sedentary/Immobility – The World Health Organization (WHO) attributes approximately 2 million deaths per year to physical inactivity. Preliminary findings from a WHO study suggest that sedentary lifestyle is one of the ten leading causes of death and disability in the world.30
Physical inactivity increases mortality (from all causes), doubles the risk of cardiovascular disease, type II diabetes, and obesity. It also increases the risks of high blood pressure, lipid disorders, and depression.30 These are known as “underlying conditions” that contribute to vulnerability.
A Korean health study found longer sitting time is associated with lower health-related quality of life and shorter sitting time with higher health-related quality of life.31 Regular exercise can reduce stress and improve sleep. It can improve regulation of the immune system and delay the onset of immunosenescence (immune dysregulation associated with aging).32
Poor sleep – Sleep problems are common in older adults. Typical symptoms include difficulty falling asleep and maintaining sleep, early-morning awakening, and excessive daytime sleepiness.33

While sleep problems may be common, it’s important to note that common does not mean “normal”. Like many other problems associated with aging, sleep problems are not an inherent part of aging.36 Many older adults have good sleep quality until the end of their lives.
Let me connect the dots between several of the factors previously discussed: Stomach acid is needed to break down proteins into amino acids. Without stomach acid, you might lack amino acids like cysteine to make glutathione or tryptophan to make serotonin. Serotonin is a mood-enhancing neurotransmitter that is a precursor to melatonin, the sleep hormone. If you have insufficient serotonin, you’ll likely be anxious and depressed, and with insufficient melatonin, you won’t sleep well. Since serotonin and melatonin are made while you’re sleeping, you’re in a vicious cycle. Without testing neurotransmitters or hormones, your conventional doctor may prescribe an antidepressant, which doesn’t increase serotonin, but rather makes it hang around longer. He/she might also prescribe a sleeping aid. Now you’re on the prescription merry-go-round.
Sleep problems have a root cause such as
- decreased melatonin production
- nocturia (the need to wake and pee at night)
- poor sleep habits such as irregular sleep-wake times, daytime napping, eating, or watching TV before bed
- caffeine
- alcohol
- medications
- restless legs syndrome
- periodic limb movement disorder
- sleep apnea
- insomnia.
Unfortunately, the above problems often go unrecognized and undertreated. It’s important to identify the root cause of disrupted sleep. Untreated sleep apnea can have serious cardiovascular, pulmonary, and central nervous system effects. In persons with dementia, severe sleep disruption can lead to nursing home placement.33
Loneliness/Isolation – My parents moved into an assisted living facility in February. It wasn’t something they wanted to do, but it was the necessary thing to do. The timing couldn’t have been worse because their assisted living facility is on lockdown now so no one can go visit them. They miss their home and the grandkids, and th

According to a University of California at San Francisco study conducted before the Coronavirus quarantine, 43% of seniors regularly experienced loneliness. The study concluded that loneliness is a risk factor for poor health outcomes including physical and/or cognitive decline and death.37
Other research links loneliness with depression, poor sleep quality, impaired executive function, accelerated cognitive decline, unfavorable cardiovascular function, and impaired immunity.38
Life can be tough for anyone who’s lost his/her sense of purpose in life. My mother’s mobility is limited, but when they lived at home, she could still do some household chores and did laundry every day for just her and Dad. We joked about her obsessive need to do laundry, but it gave her something to do that made her feel useful. In the assisted living facility, she no longer does the laundry, cooking, or cleaning. That might sound great to you, but she’s bored and not happy.
Exploring new things, being creative, and practicing gratitude can help combat loneliness. If you know an elderly person, please reach out to them regularly, if not daily, until the quarantine ends. Once the quarantine is over, please join him/her for a meal as often as you can.
Modifiable Vulnerability
Bodily decline creeps like a vine. Without proactive measures to combat the creep, it can spread like ivy in Oregon, engulfing your body. Clearly, perfect health is not a realistic expectation in old age. I hope, however, you can see how so many factors that make people vulnerable are modifiable. I hope this information can also help you see how an unhealthy diet and lifestyle contribute to disease.
Life for older people can and should be better than it is today. We are not adequately prepared for the silver tsunami. In his book Being Mortal, Atul Gawande MD shares his wisdom about aging. According to Gawande, “It’s not death that the very old tell me they fear. It is what happens short of death – losing their hearing, their memory, their best friends, their way of live…Old age is a continuous series of losses.”
So, what to do? First, acknowledge that if you do what you’ve always done, you’ll get what you’ve always got.
“The definition of insanity is doing the same thing over and over again and expecting different results.” ~Albert Einstein
There’s no quick fix, but just as health is destroyed one donut or cigarette at a time, it can be improved one step at a time – one healthy meal, one walk, one glass of water, or one supplement at a time. You can catch a virus from someone else, but you can’t just catch good health. You must choose it and take action to achieve it.
“it is important for us to remember that COVID- is a lifestyle disease that is remediated by the way we live, act, eat and socialize…We will always be confronted with communicable viruses. It is how we as a global EACH manage our environment, lifestyle and social structure that determines its pathogenicity.” ~Jeffrey Bland MD, the father of functional medicine
Remember I said your immune system is more important than the contagiousness of a virus? Dr. Bland is saying that lifestyle choices determine how pathogenic a virus is because your lifestyle choices determine how resilient you are. Your lifestyle choices affect your immune system and can make you vulnerable or resilient at any age.
“The best time to plant a tree was 20 years ago. The second best time is now.” ~Ancient Chinese Proverb
None of us are getting out of here alive. The statistical odds of death are still 100%. We each get just one life, one body, and one brain to decide what to do with that body.
God willing, if you’re not elderly now, you will be someday. You must decide which is more important: the number of years in life or the quality of life. For me quality is a clear choice and I know that a healthy diet and lifestyle are the best insurance for maintaining quality of life. I pray that you will use this knowledge to add more quality to your life – more productive and enjoyable years – more joy.
Deficiencies and insufficiencies can be corrected. Your diet and lifestyle can be modified. You are in control of what you do with this knowledge. Forward momentum is all that’s required to start living a healthier life now.
If you’ve made it through to the end of this article, congratulations! I would like to gift you with a free strategy session to help you:
- Create a sense of clarity about the health you really want to have.
- Discover the essential building blocks for having the health of your dreams.
- Determine the #1 thing stopping you from having the health you desire.
- Know EXACTLY what to do next to create the health you truly want.
Click here to book your session.
[et_bloom_inline optin_id=”optin_5″]
Disclaimer: I am a nutritionist with a Master of Science in human nutrition and functional medicine, and a research writer and editor. I am not a doctor or pharmacist. This information is for informational purposes only. You should not rely on this information as a substitute or replacement for professional medical advice, diagnosis, or treatment. These statements have not been evaluated by the Food and Drug Administration. If you have any concerns or questions about your health, you should always consult your health-care practitioner. Do not stop taking any medications based on the information presented herein without talking to your doctor.
References:
- Rochon PA, Gurwitz JH. “Optimising drug treatment for elderly people: the prescribing cascade”.BMJ. 2007; 315(7115): 1096-1099.
- https://www.cdc.gov/nchs/data/hus/2018/038.pdf
- Lee EA, Brettler JW, Kanter MH, et al. Refining the definition of polypharmacy and its link to disability in older adults: Conceptualizing necessary polypharmacy, unnecessary polypharmacy, and polypharmacy of unclear benefit. Permante Journal. 2020; 24:18.212.
- Ponte ML, Wachs L, Wachs A, Serra HA. Prescribing cascade. A new way to evaluate it. Medicina (Buenos Aires) 2017; 77:13-16.
- Mospan CM. Drug-Induced Nutrient Depletions: What Pharmacists Need to Know. US Pharm. 2019; 44(12):18-24.
- Pelton L, Hawkins K. Drug-Induced Nutrient Depletion Handbook. Lexi-Comp; 2nd Ed.,2001.
- Youssef DA, Miller CW, El-Abbassi AM, et al. Antimicrobial implications of vitamin D.Dermatoendocrinol. 2011;3(4):220–229.
- Zosky GR, Berry LJ, Elliot JG, James AL, Gorman S, Hart PH. Vitamin D deficiency causes deficits in lung function and alters lung structure. American Journal of Respiratory and Critical Care Medicine. 2011 May 15; 183(10):1336-43.
- Bjelakovic G, Gluud LL, Nikolova D, et al. (2014). Vitamin D supplementation for prevention of mortality in adults. Cochrane Database of Systematic Reviews, 2014 Jan 10; (1):CD007470.
- Prabhala A, Gary R, Dandona P. Severe myopathy associated with vitamin D deficiency in western New York. Arch Intern Me 2000; 160:1999-1203.
- Rayssiguier Y, Durlach J, Gueux E, Rock E, Mazur A. (1993). Magnesium and ageing. I. Experimental data: importance of oxidative damage. Magnesium Research, Dec; 6(4):369-378.
- Barnett JB, Hamer DH, Meydani SN. Low zinc status: a new risk factor for pneumonia in the elderly? Nutrition Reviews. 2010; 68(1):30–37.
- Haase, H., Rink, L. The immune system and the impact of zinc during aging. Immunity & Ageing2009; 6,9.
- Meng X, Li Y, Li S, et al. Dietary Sources and Bioactivities of Melatonin.Nutrients. 2017; 9(4):367. Published 2017 Apr 7.
- Zeitzer JM, Daniels JE, Duffy JF, et al. Do plasma melatonin concentrations decline with age? The American Journal of Medicine. 1999 Nov; 107(5):432-436.
- Minich DM, Brown BI. A Review of Dietary (Phyto)Nutrients for Glutathione Support.Nutrients. 2019; 11(9):2073. Published 2019 Sep 3.
- Sekhar RV, Patel SG, Guthikonda AP, et al. Deficient synthesis of glutathione underlies oxidative stress in aging and can be corrected by dietary cysteine and glycine supplementation.Am J Clin Nutr. 2011; 94(3):847–853.
- Nguyen D, Samson SL, Reddy VT, Gonzalez EV, Sekhar RV. Impaired mitochondrial fatty acid oxidation and insulin resistance in aging: novel protective role of glutathione. Aging Cell. 2013 Jun; 12(3): 415-425.
- Tsai S, Clemente-Casares X, Zhou AC, et al. Insulin Receptor-Mediated Stimulation Boosts T Cell Immunity during Inflammation and Infection. Cell Metabolism. 2018 Dec 4; 28: 922–934.
- Prescription Acetaminophen Products to be Limited to 325 mg Per Dosage. Center for Drug Evaluation and Research – https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-prescription-acetaminophen-products-be-limited-325-mg-dosage-unit. Published February 7, 2018. Accessed April 14, 2020.
- L H Block, A Georgopoulos, P Mayer, J Drews; Nonspecific resistance to bacterial infections. Enhancement by ubiquinone-8.Journal of Experimental Medicine. 1978 Nov 1; 148 (5): 1228–1240.
- Folkers K, Wolaniuk A. Research on coenzyme Q10 in clinical medicine and in immunomodulation. Drugs under Experimental and Clinical Research. 1985; 11(8):539-45.
- Folkers K, Morita M, McRee J Jr. The activities of coenzyme Q10 and vitamin B6 for immune responses. Biochem Biophys Res Commun. 1993; 193:88-92.
- Bliznakov EG. Immunological senescence in mice and its reversal by coenzyme Q10. Mechanisms of Ageing and Development.1978 Mar; 7(3):189-97.
- Weverling-Rijnsburger AW, Blauw GJ, Lagaay AM, Knook DL, Meinders AE, Westendorp RG. Total cholesterol and risk of mortality in the oldest old. Lancet. 1997 Oct 19; 350(9085):1119-23.
- Holloway RH, Dent J. Pathophysiology of gastroesophageal reflux. Lower esophageal sphincter dysfunction in gastroesophageal reflux disease. Gastroenterology Clinics of North America. 1990 Sep; 19(3):517-35.
- Maes ML, Fixen DR, Linnebur SA. Adverse effects of proton-pump inhibitor use in older adults: a review of the evidence.Therapeutic Advances in Drug Safety. 2017; 8(9):273–297.
- Nicolaidis S. Physiology of thirst. In: Arnaud MJ, editor.Hydration Throughout Life. Montrouge: John Libbey Eurotext; 1998. p. 247.
- https://www.mayoclinic.org/diseases-conditions/dehydration/symptoms-causes/syc-20354086. Accessed April 14, 2020.
- World Health Day. https://www.who.int/docstore/world-health-day/2002/fact_sheets4.en.shtml
- Kim Y, Lee E. The association between elderly people’s sedentary behaviors and their health-related quality of life: focusing on comparing the young-old and the old-old. Health Qual Life Outcomes. 2019; 17(131).
- Neiman DC, Wentz LM. The compelling link between physical activity and the body’s defense system. Journal of Sport and Health Science. 2019; 8(3):201-217
- Neubauer DN. Sleep problems in the elderly. American Family Physician. 1999 May 1; 59(9):2551-2558.
- Besedovsky L, Lange T, Born J. Sleep and immune function.Pflugers Arch. 2012; 463(1):121–137.
- Villafuerte G, Miguel-Puga A, Rodriguez EM, Machado S, Manjarrez E, Arias-Carrión O. Sleep deprivation and oxidative stress in animal models: a systematic review. Oxidative Medicine and Cellular Longevity. 2015; 2015:234952. Epub 2015 Apr 6.
- Rodriguez JC, Dzierzewski JM, Alessi CA. Sleep problems in the elderly.Med Clin North Am. 2015; 99(2):431–439.
- Perissinotto CM, Stijacic Cenzer I, Covinsky KE. Loneliness in older persons: a predictor of functional decline and death. Archives of Internal Medicine. 2012 Jul 23; 172(14):1078-83.
- Hawkley LC, Capitanio JP. Perceived social isolation, evolutionary fitness and health outcomes: a lifespan approach. Philosophical Transactions of the Royal Society B. 2015 May 26; 370(1669).